A quiet young woman, curly dark hair parted in the middle and pulled back in a bun, sat in the corner of the classroom with her book in front of her and said almost nothing the entire semester. But she was listening.
I would like to shine a light on Ebelyn Garcia, my surprising student from Environmental Literature, and my very first guest blogger. In her essay + poem + letter to her parents, she declaims the unfairness of poisoning people who have no way to know they are being poisoned, of hiding the truth of widespread health risks in the secret recesses of our very own bodies. Articulate and authentic, she argues that it is important to "be loud so these systems that allow this” can be countered and overcome.
You see, her parents have built their lives around a landscaping company and work with these chemicals every day. Her quiet voice represents not only her, but the millions of people exposed without their knowledge and consent to chemicals linked to cancer, neurocognitive deficits, infertility, autoimmune disease, and more. This is how some people feel when they realize that those they have trusted to protect them have utterly failed, have profited from the diseases of the uninformed and preyed upon the silence enforced by the corporations that produce these toxic products.
And so I pass on to you the gift of Ebelyn’s formerly silenced, now loudly resounding voice.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Ebelyn Garcia
Environmental Literature
04/13/2026
Anyone who is not informed about illnesses thinks that they are caused by genetics or personal choices. Although those things play a huge role, that is not always the case. Environmental pollution and chemical exposure have a serious say in human health, but there's rarely much about that in conversations about diseases.
Reading Living Downstream was a wakeup call. In my day-to-day schedule, there are classes that have a lab included, and I spend a good amount of time looking at cells. Sandra Steingraber drilled into my head that cancer is not always genetic. Many products we use or even buy in stores have many chemicals that we aren't aware of.
We need to use science to not only treat disease but to also prevent them. Living Downstream changed the way I now look at health. I always thought genetics or personal lifestyle choices cause cancer, but a polluted environment can cause illness, including cancer. This changed the way I think about my health. As a biology student and woman, the book made me reflect on the chemicals that aren’t talked about in our daily products; there's a big lack of awareness about these toxins that may affect hormones and long-term health, and the importance of using science not only to treat illness, but to prevent it.
When the subject of cancer comes up, I feel empathy for those having to change their life around due to cancer affecting them and their family, but I don’t think they are less than others. I believe they are going through this battle for a reason, and whether they survive or not, they leave an important message to their loved ones. I ask myself if the person has been smoking throughout their life, or were they exposed to smoke, because although it was hard for me to believe that being exposed to smoke causes cancer, it’s true. But no one thinks environmental chemicals contribute to cancer.
Steingraber explains how pesticides, industrial chemicals, and polluted air will cause cancer over time. She used science and her own experience as a cancer survivor; she made this feel so much more personal – it felt like a warning to humans. She emphasized how important it is to prevent these illnesses by figuring out what is harmful. She wrote “We are all downstream now.” We all live in this environment together. Chemicals are released every day and will later on affect everyone's health. These are health risks, and not many people have control to stop it. She wants us to not just focus on treatment for cancer or any illness, but to look for ways to prevent it by identifying what truly harms our bodies and taking action before we cause more damage to ourselves.
When reading Living Downstream and realizing that those harmful chemicals are everywhere, including factories, I realized that they are present in my everyday products. Any cosmetics, lotions, cleaning products and even perfumes all can contain chemicals. Everyone thinks since it's sold at a store with closed lids and you are the first person to open it, it's completely safe to use, but the book suggests that exposure to low levels of different chemicals will affect the body over time, causing disruption of hormones.
In my Environmental Literature class, my professor, Dr. Kauth, has inspired me to look at the world in a more realistic way. She mentioned extra credit to go watch a new documentary that recently came out on Netflix, The Plastic Detox (2026). In this film, there were six couples wanting to become parents, but there was an issue of infertility due to how much plastic was in their bodies. It affected their fertility rates and made it almost impossible to have kids. Shanna H. Swan is the expert in this experiment and studied how plastic affects health and in this case fertility. She did an experiment with six couples who have been trying to bring a baby into the world but failing, and even doctors didn’t have an answer on what the issue was. Swan guided the couples in cutting plastic out of their lives for a couple months, and she explained how the chemicals in plastics can affect hormones. Plastics are everywhere because of how cheap they are, and our government hasn't taken action on reducing plastics because industry only gets richer from it. After a few months, the couples had lower levels of chemicals in their bodies, and some men improved their sperm quality. Three couples got pregnant. This shows how plastics are everywhere, including inside our bodies. So many chemicals that we are unaware of are constantly being inhaled and consumed by humans, and that has a lot to do with our lifestyles and our environment.
Both Plastic Detox and Living Downstream helped me view the issues that no one really talks about. This becomes so personal because it's our health. Chemicals have really taken a huge role in our daily lives; they are working quietly in our bodies, affecting hormones. Watching the couples trying their best to get rid of plastic makes me want to act fast and attempt to better my home, not only for me but for my family: my parents who are getting older and older, my little sister who has a bright future ahead of her, and my brothers who work long hours and use plastic containers for their lunch because it’s fast and easy to store food.
Chemicals are in my kitchen and bathrooms, and we are not going to let those chemicals harm us. They will not mess with our reproductive health. Now I know the things I use every day contain so many harmful chemicals, they trick the human body by blocking estrogen, which can affect my menstrual cycle and fertility. It all feels like a secret. We need to raise our voices and be loud so these systems that allow this can help get rid of it instead. Staying healthy, of course, is watching what we eat, but also swapping out what’s needed. We need to stand our ground and push for a world that cares about our health over money.
Secret
My body is mine.
It heals on its own.
It's a system that always knows what to do.
No one seemed to know about the secret
the invisible guest entering my body
little by little,
affecting my health.
My blush, my lip gloss, my lotion, and my plastic water bottle
I never leave behind.
No one told me plastic speaks.
It invades my hormones,
pretending to be something it’s not.
Does my body distrust me for causing so much harm?
Cycles are interrupted.
Estrogen becomes confused.
Do I still have a future?
I wonder about the women before me
The illnesses with no reason,
things too small to see.
A SECRET?
I live here, wrapped in plastic.
Now I notice
The plastic container,
The plastic packaging,
The plastic toys,
My plastic toothbrush,
My plastic bottle for my shampoo,
My plastic water bottle,
My reusable plates,
My harmful pans,
My favorite perfume,
My everyday lotion,
The labels with small letters.
And most importantly, the health of my father
A hard-working landscaper who came from nothing to owning his own company.
If I, who went to school all my life, am now barely finding out about this secret,
How will my father know? Who stopped going to school in fifth grade!
It’s my job to not keep this secret.
It’s invisible,
but it has a name.
We will challenge it.
And we will make a change.Ebelyn Garcia
Dear Mom and Dad,
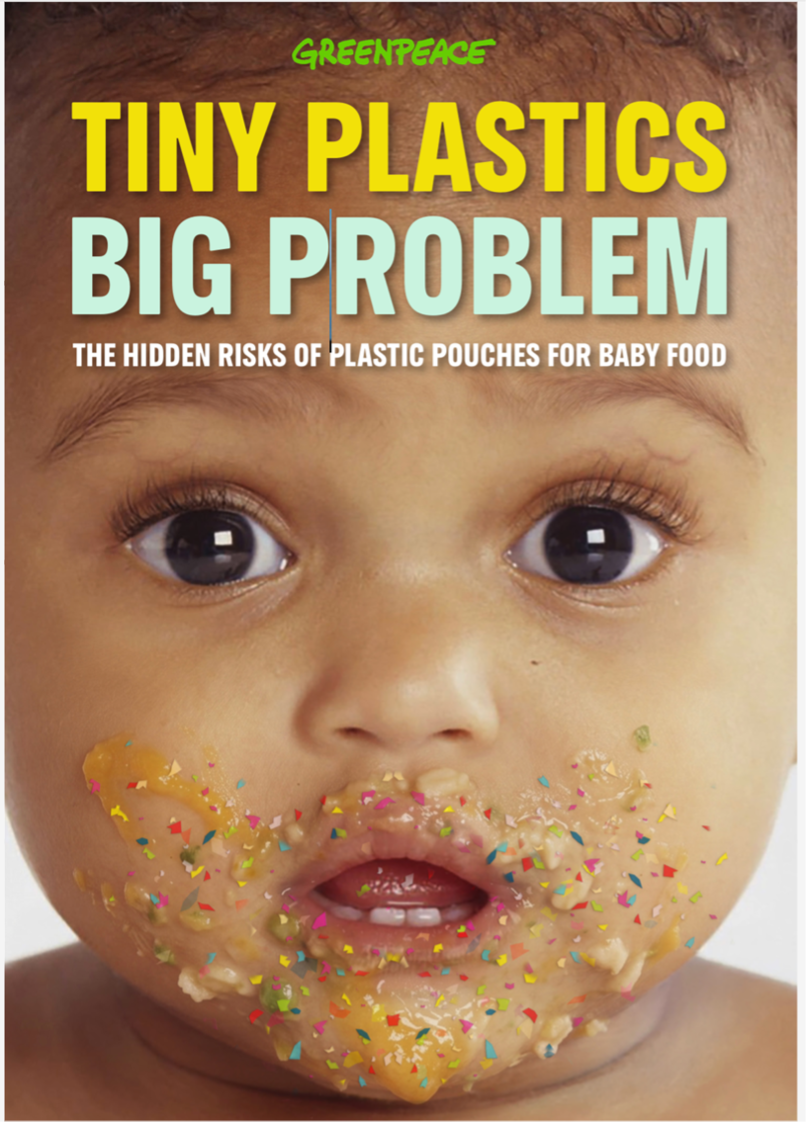
I know there's so much going on in this paper and so much information, but I hope you made it this far. I will use easy words for you to easily understand me. I’ve discovered how harmful plastics and chemicals are to us. They harm our bodies without us even knowing. We use them every day, and we don’t think twice about it. Yes, it’s easier to grab a plastic water bottle or plastic Tupperware for lunch breaks, but we are clueless about what’s in the plastic. There are tiny little microplastics that can affect our hormones or cause illness over time. This changed the way I see everything, and I believe it should change your mind too.
This made me think about my future, all the kids I want to have, and your health. I wonder how many people suffered because of this and never discovered that all of this was an issue related to their illness. Mom and Dad, you have worked so hard your entire life to provide a better future for my siblings and me. Both of you came from nothing to building this landscaping company together, from working minimum wages to being business partners. Your hard work is recognized all the time.
As someone who has been in school for so long, I am only now learning about the dangers that no one talks about, so how could you know? Dad, there are so many chemicals you work with daily – the plastic water bottles, Gatorade bottles, any other drinks you keep cool for you to hydrate yourself – they are all harming you. It's convenient to use, but it's not worth your life. We can together move step by step to get rid of all this. It doesn’t have to be done all in one day – that's impossible. We can look for a replacement of those chemicals you use. The machinery, I know, is expensive, but at least consider wearing a mask while you use it. The boots you bring into the house – consider leaving them outside before you enter. There are so many little steps we can take starting now.
Mom, little by little, let go of the pans that harm us, the plastic plates, Tupperware, cutting boards, the lotions or shampoos that you use. Start a good habit of reading the labels on the products you use. The book that I keep mentioning has helped me open my eyes and realize how harmful chemicals, pesticides, and polluted air will cause cancer over time. Cancer is not just about genetics; it's not just because you smoke tobacco. It can be because of how much we contaminate our earth. As humans, we need to take care of it because we only have one Earth.
Although environmental literature did sound a little boring, I will admit it’s one of the most eye-opening classes. I was intrigued with the books we read. I'm truly thankful to my professor, Dr. Kauth, for allowing us to learn about what harms us and our environment. We can do this together, and we can start by preventing people from using any chemicals, anything that harms the environment and humans, and the same for plastic – we need to reduce it from our lives. I want us to look at the small things, ask questions if we have to, and overall protect ourselves and everybody around us as much as we can. It's obvious we cannot avoid everything, but taking little steps matters.
Our health to me is so important, especially your health. I believe it's so unfair how we are not informed about the environment that we live in. It's our job to inform the people around us of what we know. I didn't just write this because it's an essay I have to turn in for a grade. I wrote this because I truly love you both, and I believe we can all learn together and take good care of our bodies – of course little by little because we are humans, and we aren't perfect. This makes me appreciate everything you sacrificed so much more. I now see the meaning of everything you sacrificed so my siblings and I could have an education. I want to use that education to help others. Maybe these chemicals are invisible, but they have a name, and they can be challenged.
References
The Plastic Detox. (2026). https://www.netflix.com/title/82074244.
Sandra Steingraber. Living Downstream. Da Capo Press, 1997.